
Will the Real ACIP Please Stand Up?
How the politicization of vaccine policy is threatening public health and why understanding the ACIP’s origins matters now more than ever.

I’m David Higgins, a practicing pediatrician and preventive medicine physician who cares for children, adolescents, and their families and studies how to improve how we communicate about and deliver preventive care and vaccines. This newsletter shares clear science, smart policy, and meaningful conversations, because the health of our communities depends on all three. If you haven’t already, hit the button below to stay in the loop with updates.
Hi Community,
The draft agenda for the first meeting of RFK Jr.’s handpicked vaccine panel—formerly the Advisory Committee on Immunization Practices (ACIP)—was released. And it’s exactly what many of us feared.
A Familiar Conspiracy Theory, Now with Federal Backing
The agenda includes a presentation “regarding thimerosal in vaccines” with the presenter TBD, and a vote for “thimerosal containing influenza vaccine recommendations”. Concerns about thimerosal in vaccines are not new. Vaccine cynics repeatedly want to relitigate this, despite it being removed from vaccines in the U.S. (except for a tiny sliver of influenza vaccines) for decades, and extensive research showing thimerosal in the levels found in vaccines does not cause significant harm.
Another unplanned, but perhaps predictable, addition is time set aside to revisit the use of the MMRV (measles, mumps, rubella, and varicella) vaccine in children under five. While I have theories, the direction of this is unclear. What is clear is the playbook: reintroduce long-settled fears about vaccine safety, autism, and “toxins”, all topics that anti-vaccine groups have spent years reviving.
They’re not offering new evidence; they’re just playing their greatest hits on a reunion tour.
What’s Missing Is Just As Alarming
Equally concerning is what is missing from this meeting agenda, which doesn’t align with what was posted in the Federal Register:
Career CDC Staff who have historically organized, presented, and provided critical expertise at ACIP meetings are now absent.
Several key discussion items are either postponed or removed. The agenda omits updates on CMV, HPV, meningococcal, pneumococcal, and adult RSV vaccines.
Planned votes on HPV, meningococcal, and adult RSV vaccines have vanished without explanation.
Several agenda items, including those on thimerosal, MMRV, and COVID-19 vaccine safety, list presenters as “TBD.” That raises major concerns about who will provide input on these important topics.
Whether intentional or not, the strategy seems twofold: to resurrect long-debunked controversies and delay progress on urgently needed vaccines.
Others Are Stepping In. But It’s Not a Long-Term Solution
In the wake of ACIP’s dismantling, professional societies, advocacy organizations, and state governments are stepping up.
Many organizations have made strong statements opposing these events. And I expect in the coming weeks, we will see these groups, and the hundreds of thousands of clinicians and scientists they represent, make it clear they will not sit quietly while decades of evidence-based policy is unraveled.
In a recent Washington Post op-ed, Dr. Ashish Jha called on states and medical societies to assert their own authority to recognize and implement evidence-based vaccine guidance.
In Colorado, I was part of efforts to pass two landmark laws that ensure state vaccine policy and insurance coverage don’t rely solely on federal bodies like RFK Jr.’s panel. These laws allow for expanded guidance from trusted sources like the AAP, AAFP, etc. I had hoped we’d never need them. Now I’m grateful we acted when we did. Read my interview with Colorado Public Radio, which breaks these down more.
This patchwork approach is not ideal. Access to affordable and convenient vaccines should not depend on the state or region you live in. That is why a strong, science-driven federal advisory body matters.
Understanding How We Got Here
So, how did we get the ACIP in the first place?
To answer that, I’m launching a two-part series on the origins and evolution of vaccine recommendations in the U.S. I hope this history helps you understand why the ACIP is important and why replacing it with a patchwork of states, organizations, and other committees cannot be a long-term solution.
If you’re curious (or just a history nerd like me), join me for Part 1 below.
Part 1: A Look Back: Who Made Vaccine Recommendations Before ACIP?
Long before there was an Advisory Committee on Immunization Practices (ACIP), vaccine guidance in the United States came from pediatricians.
In 1933, the American Academy of Pediatrics (AAP) established a “Special Committee on Prophylactic Procedures Against Communicable Diseases.” Two years later, that committee published a six-page document titled Routine Measures for the Prophylaxis of Communicable Diseases—the ancestor of today’s Red Book (which every pediatrician keeps handy on their shelf!). This early document offered guidance on vaccines and preventive strategies for diseases like diphtheria, typhoid, whooping cough, measles, smallpox, polio, rabies, and tetanus.
By 1936, the AAP formalized this work by creating the “Committee on Immunization Procedures,” later renamed the “Committee on Infectious Diseases.” This committee—still active today—has long been comprised of pediatricians and experts in infectious diseases, vaccinology, and public health who continue to guide the AAP’s vaccine recommendations.
From 1939 through 1947, this committee updated and republished its guidance to reflect fast-moving scientific advances. Between 1948 and 1964, the Red Book was the country’s primary source of immunization recommendations.
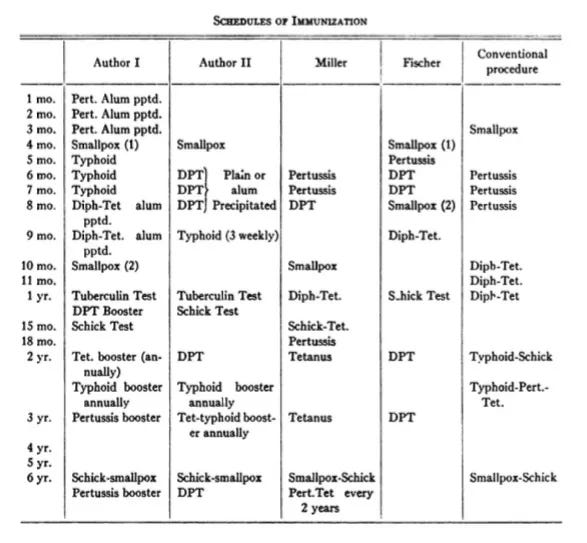
Contrary to anti-vaccine mythologies, kids in the 1940s and 1950s did get vaccinated, often with vaccines that had more side effects and delivered more antigens than today’s improved formulations. We’ve made enormous progress in vaccine safety and technology. The idea that vaccination was somehow simpler or safer in “the good old days” doesn’t hold up.
Why the ACIP Was Created

The 1944 Public Health Service Act gave the U.S. Surgeon General authority to recommend vaccines for licensure. But in the 1950s, the pace of vaccine innovation skyrocketed. Federal guidance couldn’t keep up. Public Health Service-issued recommendations for polio and influenza vaccines began appearing in 1960, and temporary expert committees were convened (e.g., for polio in 1962, measles in 1963).
But this piecemeal, one-vaccine-at-a-time approach wasn’t working. And as the 1964 ACIP meeting minutes noted, existing vaccine guidance was fragmented:
While the AAP was the leader in vaccine recommendations, it was focused on pediatric care.
The Armed Forces Epidemiological Board gave vaccine recommendations, but focused on military populations.
The American Public Health Association issued guidance for the U.S. and parts of the world, but this was infrequent, occurring every five years.
In minutes of the first ACIP meeting, they noted:
“None of these committees is directly concerned with providing advice on a concurrent basis regarding the effective application in public health practice of agents for communicable disease control purposes. It is hoped that the Advisory Committee on Immunization Practice may fulfill this function.”

No committee addressed the broader public health application of vaccine policy in real-time. That’s why ACIP was created—to ensure national, timely, population-focused recommendations rooted in science and implementation realities.
However, they never intended to do this alone. Even at its first meeting, the ACIP emphasized collaboration, including formally discussing its relationship with the AAP’s Red Book Committee. Since then, it has collaborated regularly with dozens of organizations and stakeholders.
Why This Matters Now
ACIP’s structure was intentionally designed to balance rigorous evidence review with practical guidance for real-world delivery. It worked. For six decades, it guided the U.S. through pandemics, new vaccine rollouts, and immunization updates.
But now, it faces an existential threat, not because of scientific failings, but because of political interference.
Fragmented recommendations will breed confusion, erode public trust, and undermine the equitable access and coordination that our unified national recommendation system was built to ensure. While state and organizational efforts may be necessary in the short term, replacing the ACIP with a patchwork of competing and potentially conflicting guidance is not a viable long-term solution.
The ACIP model isn’t perfect, but it has served the public for 60 years with scientific rigor. If we let it be replaced by ideology, the consequences will fall hardest on the communities already struggling to access vaccines.
We owe it to the legacy of public health and to every child whose future depends on it not to let that happen.
Thanks, as always, for being part of this community. I know there’s a lot going on, so I’ll keep tracking the headlines that matter and unpacking what they mean so you don’t have to.
-David
Do you like this newsletter?
Then you should subscribe here for FREE to never miss an update and share this with others:
You can also follow me on LinkedIn, Instagram, Substack Notes, and Bluesky.
Community Immunity is a newsletter dedicated to vaccines, policy, and public health, offering clear science and meaningful conversations for health professionals, science communicators, policymakers, and anyone who wants to stay informed. This newsletter is free for everyone, and I want it to be a conversation, not just a broadcast. And if you find this valuable, please help spread the word!
References
Want to dig deeper? Here are the sources I used for the history section of this article—real references, reviewed by a real human (not hallucinated by AI). I hold myself to higher standards than that:
Pickering LK, Peter G, Shulman ST. The Red Book Through the Ages. Pediatrics. 2013;132(5):898-906. doi:10.1542/peds.2013-2538. Link
Walton LR, Orenstein WA, Pickering LK. The history of the United States Advisory Committee on Immunization Practices (ACIP). Vaccine. 2015/01/09/ 2015;33(3):405-414. doi:https://doi.org/10.1016/j.vaccine.2014.09.043. Link
Minutes, meeting no. 1, Advisory Committee on Immunization Practices, May 25-26, 1964. Corporate Authors(s) : Communicable Disease Center (U.S.). Advisory Committee on Immunization Practices. Conference Author(s) : Communicable Disease Center (U.S.). Immunization Practices Advisory Committee. Meeting (1 : May 25-26, 1964 : Atlanta, GA). Published Date : July 6, 1964. Link
https://historyofvaccines.org/getting-vaccinated/vaccines-children/development-immunization-schedule
Hinman AR, Orenstein WA, Schuchat A; Centers for Disease Control and Prevention (CDC). Vaccine-preventable diseases, immunizations, and MMWR--1961-2011. MMWR Suppl. 2011;60(4):49-57. Link
Hi Dr. Higgins! I am disappointed upon hearing that a part of the upcoming ACIP's meeting agenda is to revisit some of these already defunct or disproven statements. Revisiting such statements do NOT help people including ones who experienced common and rare side effects. For the record, I support vaccination wholeheartedly because it protects people way better than its predecessor, which is variolation. I do want the vaccination technology to be improved so that it's much easier for the country to combat different diseases. I am even more disappointed that there are other critical items missing from the meeting agenda; that's very bad.